Blogs
Prostate Cancer: My Story
Introduction
At the end of 2010, my GP requested a round of blood tests, which is pretty normal for someone in my age group. He is very thorough and felt that some things now needed to be checked annually. One of the things that worried him from the tests was that my PSA level was 3.8, which was high for my age at the time, but not excessive. He arranged for me to visit a urologist to investigate this further.
First biopsy
The urologist carried out a physical examination, including a digital rectal examination. The examination was inconclusive, so he felt that a prostate biopsy was necessary. The biopsy was carried out, and the night after the biopsy was the most awful of my whole life - I have never experienced such pain. The only place that I was comfortable was sitting on the toilet as nothing was in contact with my rectal region. When I got to see the urologist, a couple of days after the pain subsided, he said it was a haematoma in one of the seminal vesicles (I was told the chances of this happening is greater than 106:1 - although the article from Nature linked above suggests otherwise). He recommended that I have it drained, and as he was going to be away, he recommended that one of his colleagues do the job.
Of course, this entailed another full examination by the new urologist, including a digital rectal exam. It also entailed another surgical procedure. The irony was that by the time this occurred, the blood in the vesicle was no longer liquid, so the whole exercise was rather futile, costing a great deal of money. (There were other issues but they are of minor importance.)
Another ironical point was that the biopsy yielded no cancer. The diagnosis was thus pinned down to benign prostatic hyperplasia (BPH). Detrusitol was prescribed to try and improve urine flow. I was also told to avoid beer (my life-blood) and any other carbonated drinks. During this whole exercise, I lost 10kg in weight. Anyone who knows me, will know that this is quite a big chunk of my total body mass. However, I did stick to the no-beer rule.
Second biopsy
At the end of 2011, my PSA level was marginally higher than at the end of 2010, so my GP was happy to leave things as they were. However, at the end of 2012, it jumped to 5.3, which meant another visit to the urologist.
As before, the physical examination yielded nothing, so he called for another biopsy, which took place early in 2013. Of course, I was dreading a repeat of the haematoma, but everything went off well. The biopsy yielded nothing, so he reiterated his BPH diagnosis. He did, however, change the medication from Detrusitol to Avodart.
It was shortly after this that I decided I was missing out on too much, especially with the bowling fraternity, so decided to start drinking beer again. My decision was vindicated by the fact that my weight increased by 5kg by the end of the year. Also, my PSA level dropped with the end of year tests, showing me that beer had nothing to do with the PSA levels. At the end of 2014, my PSA level was still good and I had put back all the weight I had lost after the first biopsy.
TURP
Unfortunately, with the blood test at the end of 2015, my PSA level had jumped to more than 6. My GP decided that another visit the urologist was necessary.
After the usual physical examination, and a urine flow test, the urologist came up with his prognosis. He felt that another biopsy was not going to yield anything, but what he did recommend was that I undergo a Trans-Urethral Resection of the Prostate (TURP) to widen the passage from the urethra to the bladder through the prostate (I like to think of it as a rebore!). This was scheduled for early April 2016.
The operation was successfully completed with me then having to spend four nights in hospital. I had to have a bladder flush on the second night as the ward sister felt there was insufficient clotted blood being released into the catheter bag. On the morning when I was due to be released, I also had some fun convincing the sister that my urine was clear enough for her to sign the final release form!
Cancer
With the follow up visit to the urologist, I was given the bad news that cancer had been found in one of the two sections removed from the prostate. He said it was very small, and with luck he had removed it all with the TURP. He did, however, call for a bone scan, just to be certain that the cancer had not metastasized. Fortunately, the scan was clear. He called for a PSA check six months down the line.
Unfortunately, that PSA test result was bad - it had jumped to over 8. His recommendation was that the prostate be removed by robotic surgery. The alternatives being the normal "bikini-cut" surgery or beam radiation therapy. He did omit to mention brachytherapy as another alternative (one which I might have chosen in hindsight). The advantage of the robotic surgery is that the time spent in ICU and in hospital was very much less than with normal surgery. The other advantage being that the catheter can be removed within 10 days of the operation.
Now I know how much hassle both Willie and John went through with their normal prostatectomies, so I wasn't too interested in that. Having worked in the nuclear industry, made me not very keen on beam radiation therapy. My GP agreed with me on this. He said he had two patients who had had beam radiation therapy and both were suffering from radiation damage to the rectal region of the colon. He recommended a prostatectomy.
Pat and I had a joint discussion with the urologist and we decided that the robotic prostatectomy was the way to go. The earliest date available for both the urologist and the apparatus was early February 2017 (this was early December 2016). In the meantime, approval for the procedure had to be obtained from my medical aid (this was enough of a problem that I might devote a separate page to that).
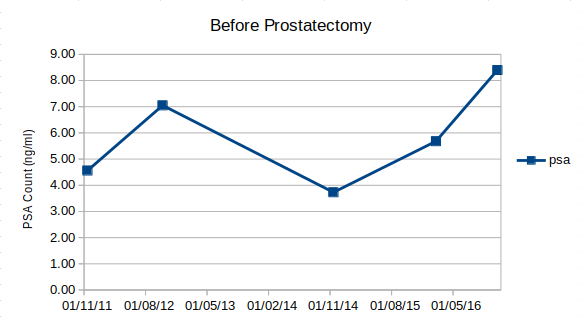
Graph showing PSA levels (unfortunately, there are some missing points)
Prostatectomy
I was admitted into the hospital the evening before the surgery was due to take place. Early the next morning (Saturday) I had to have a bath in a tincture of iodine! I was then wheeled into the theatre and was shown the da Vinci instrument by the anaesthetist. He then gave me an epidural injection and I don't remember anything after that until waking up in ICU.
In short, I was moved into a general ward before lunch on Sunday and discharged around teatime on the Tuesday after the op - a total of four nights in the hospital, three of which were post-op!
I must say the staff went out of their way to make my stay in the hospital as pleasant as possible
Recuperation
(More detail here.)
The first part of my stay at home was made difficult by urine leaking past the catheter. Pat got incontinence pads at Dlschem on the Sunday and this helped a great deal.
The urologist took the staples out on the Monday, and said he would remove the catheter on the Friday. Before he did that I had to have a cystogram to check for leaks at the bladder/urethra interface. No leaks were found and the catheter was removed on the Friday, 13 days after the op.
I had my first follow with the urologist regarding PSA results 17 weeks after the op. The level was 0.27 which I thought it was pretty low considering what it had been. The urologist however was not too happy as he felt it was too high.
Radiation Therapy
Unfortunately, my PSA count rose to 0.51 in July, and this worried both my GP and the urologist. The urologist wanted me to have a Prostate Specific Membrane Antigen (PSMA) PET scan with 68Ga as the tracer. However, the only institution in Pretoria able to do the Ga scan was the Academic/State Hospital and my medical aid was not prepared to pay for this scan. I was not too unhappy with this turn of events, as I know from having taught at the hospital, that finding parking there is a nightmare. This prompted me to look for alternative PSMA scanning facilities in Pretoria.
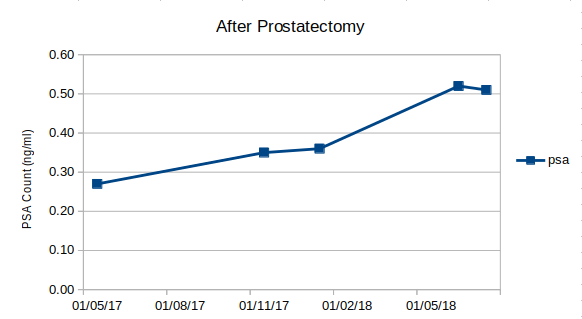
Graph showing PSA levels after prostatectomy
On chatting to Willie, he said he'd had both 68Ga and 99Tc PSMA scans and that the Ga scan had shown nothing, but the Tc one did. So, I went ahead and had the 99Tc scan.
The scan showed "Low grade Tc 99m PSMA uptake is visualized in relation to the prostate bed region". When the urologist saw this be sent me straight off to an oncologist.
After an examination (including the infamous digital rectal exam), the oncologist recommended radiation therapy.
The radiation therapy involved 6 weeks of a daily dose of x-rays focussed on the prostate region and the lymph nodes in the groin. This was incredibly boring, as there was always a long wait in the reception area of the oncology centre and the radiation treatment session itself only took less than ten minutes. One of the most interesting things to me was being shown the x-ray generator - it looked for all the world like a large quadrupole mass spectrometer!
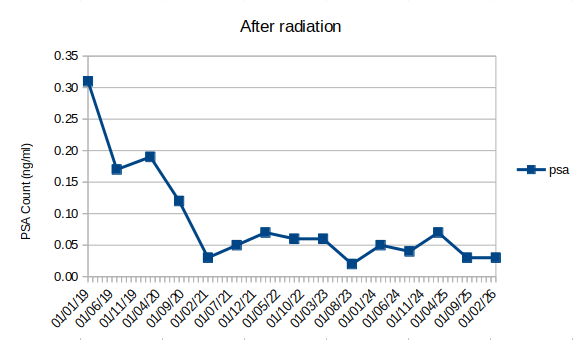
Graph showing PSA levels after radiaton therapy (updated 2 March 2026)
(December 2018)
After Radiation Therapy
If one looks at the previous graph, it certainly does look like the radiation treatment did its job, as the PSA count is now often below the detection limit of the spectrometer used to measure it.
Unfortunately, there was one unwanted side effect from the treatment - urinary bleeding (hematuria) after certain activities. The first time this occurred was a couple of months after the treatment had finished, when I was trying to clean gutters. This involved carrying (and extending) a 6m extension ladder. A couple of days after this I had a serious bout of bleeding, which stopped after a day. After this, I had several bouts of bleeding, and I have narrowed the problem down to carrying of certain objects and more often with constipation (trying to force the stool out). The oncologist was not too worried about this and said it would more than likely disappear with time (unfortunately, this has not happened after five years).
As this is probably due to radiation damage in the bladder and prostate region, any stress on this region may cause the bleeding. This is more than likely radiation cystitis (thanks René).
(7 October 2023)
Radiation Cystitis
Ironically, shortly after I updated the previous section, I was laid low by the radiation cystitis. While working on a detachable awning for my bakkie, I overdid something which triggered bleeding which would not stop. Clotting of blood in the urethra prevented me from urinating which was very painful. Pat took me to the urology hospital, where they inserted a catheter - although relief was immediate, this was the start of my latest nightmare.
In the urology hospital, flushing of the bladder was done by means of gravity (bag) irrigation. However, this seemed to bypass the clots, which had to be removed by manual (syringe) irrigation. The clot build up was extremely painful, and relief from the manual irrigation was immediate. An attempt was made to stop the bleeding through the use of silver nitrate, but this did not work due to the regular manual irrigation to reduce clot build up.
A secondary problem, due to the loss of blood, was the onset of anaemia. This was due to low haemoglobin and a worryingly low red blood cell count. I had eight blood transfusions to try and stabilise the anaemia, but the continued blood loss kept the counts low.
In order to stop urine flowing through the bladder, the urologist decided to divert the urine flow to a separate bag for each kidney (nephrostomy). The idea was that with time the bladder would have a chance to heal itself and once the healing was complete, the kidneys could be reconnected to the bladder. However, this procedure required moving me to another hospital.
The procedure was carried out almost immediately after arriving at the second hospital. An unfortunate side-effect of the anaesthetic was really bad dreams.
After three nights in High Care, the catheter was removed (great relief after seven days), and I was moved to a general ward.
The anaemia remained a problem, even though the bleeding from the bladder was much reduced. In spite of this, both the ward physician and the urologist gave me the green light to go home, four days after the procedure was carried out (after ten days in hospitals).
At home, the biggest problem was trying to combat the anaemia as this caused tiredness and a lack of energy. The use of iron and vitamin B12 supplements seemed to have helped, as both the haemoglobin and red cell counts were improved after a week. An unwanted side-effect was an increase in the platelet count. This could be due to excess silver nitrate and hopefully the platelet count will return to normal soon.
Three weeks on, the anaemia seems to be improving with all the blood counts moving in the right direction. Also, there has been no blood from the bladder for more than a week. However, the specialists feel that I should have hyperbaric oxygen to assist with the healing of the radiation cystitis. If the medical aid approves this treatment, there will be 20 one hour sessions (four weeks) in the hyperbaric chamber. I am not sure how the nephrostomy bags will work under high pressure, but it does mean another four weeks with the bags.
It has been six weeks since I left the hospital, and unfortunately, due to Christmas holidays interfering, I still have the bags. AND, the bags will be with me until the end of January when the urologist returns from leave.
The hyperbaric oxygen treatment has not happened, ostensibly as the medical aid have not given the clearance for payment (however, I have a feeling this is also to do with Christmas holidays as the treatment would have carried on to the Christmas week).
I have had to ask my GP to change the dressings covering the region where the pipes go into the kidneys, as these were starting to lift. Urine is also starting to leak past the nephrostomy tubes into the bladder, which has also become an irritation, as this leakage causes urine to drip from the penis (reminiscent of the pissiness after the prostatectomy mentioned above). I had the GP test the urine for blood from both the penis and the bags, and found that blood in the urine seems to be coming from the kidneys, rather than the bladder. The urologist's idea that the system should last until the end of January is looking less and less likely.
(15 December 2023)
As the earth continued revolving around the sun, I unfortunately forgot to continue the story about what happened with the nephrosotmy tubes!
I did manage to get through Christmas and New Year, and then a good deal of January with the bags in place.
When I saw the urologist, he was rather unhappy that I hadn't had the hyperbaric oxygen treatment, but was happy enough to give the go ahead to remove the tubes.
A few days later, the tubes were removed in his rooms and I was very happy to leave without the bags. Since the removal of the tubes, I have seen very little blood, and I think the blood that I do see is from a kidney rather than the bladder (the colour is a very pale pink rather than the deep red that I was used to). The biggest problem that I have currently is urine leakage. This is totally unlike anything I had before my time in hospital, so I have a feeling that something was damaged during the excessive amount of bladder irrigations that I had to undergo.
When reconciling the accounts in February, I found that I had actually had 12 units of blood during my hospital stay, which must mean that I had lost a lot of blood, and was pretty close to saying goodbye to the world!
(29 July 2024)
